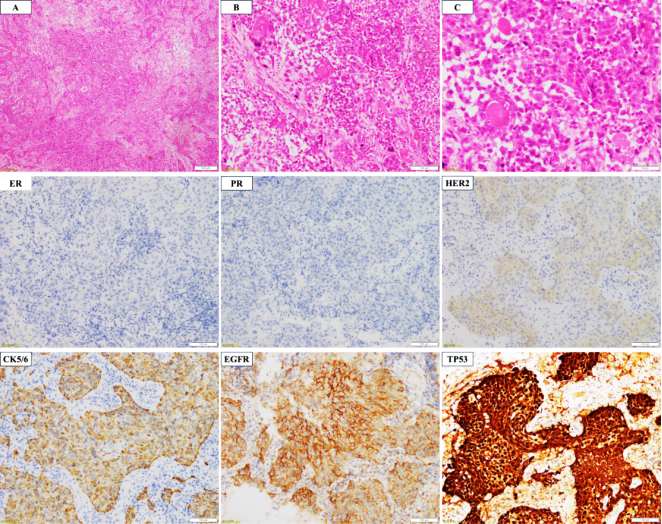
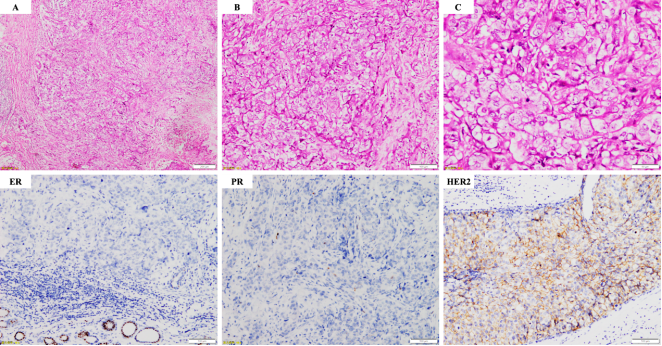
Drug resistance, recurrence, and metastasis are the main challenges that can lead to treatment failure and deteriorate outcomes of patients with breast cancer. Breast cancer metastasizes to different organs and may present with different phenotypic features. However, the underlying mechanisms of phenotypic plasticity of breast cancer still remain unclear. We herein report a case of HER2-positive breast cancer in which the patient developed acquired therapeutic resistance following standard postoperative adjuvant chemotherapy combined with anti-HER2 targeted therapy. The patient initially responded to treatment; however, one year after completion of therapy, new bilateral pulmonary nodules emerged. Subsequent pathological examination confirmed metastatic carcinoma with a transdifferentiated squamous cell phenotype. Comprehensive biomarker analyses, including immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and next-generation sequencing (NGS), were performed on matched samples from the primary breast tumor and the corresponding lung metastatic lesions. Integrated diagnostic results confirmed that the pulmonary lesions were metastatic in origin from the breast, harboring HER2 amplification as well as PIK3CA and TP53 mutations. In contrast to the primary lesion, the metastatic lung lesions demonstrated acquisition of a squamous phenotype, accompanied by multiple chromosomal heterozygous/homozygous deletions and copy-number gain that may have contributed to this phenotypic transformation. Despite HER2 amplification, the pulmonary metastases showed negative HER2 protein expression, possibly reflecting tissue-specific gene expression differences. These findings provide new insights for the clinical management of HER2-positive breast cancer.
| Published in | American Journal of Clinical and Experimental Medicine (Volume 13, Issue 6) |
| DOI | 10.11648/j.ajcem.20251306.12 |
| Page(s) | 170-176 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Metaplastic Breast Cancer, Lung Metastasis, Squamous Cell Metaplasia, Case Report
Tumor type | Gene | Exon | Nucleotide changes | Amino acid changes | Variant classification | Mutation frequency / copy number |
|---|---|---|---|---|---|---|
Invasive breast carcinoma, grade III | PIK3CA | exon21 | c.3140A>G | p.H1047R | Class I variants | 77.2% |
TP53 | exon8 | c.818G>A | p.R273H | Class I variants | 57.0% | |
ERBB2 (HER2) | - | - | - | Class I variants | 5.5 | |
ETV6 | exon6 | c.1105C>T | p.R369W | Class II variants | 14.3% | |
ZFHX3 | exon8 | c.3590C>T | p.P1197L | Class III variants | 31.5% | |
Lung tumor lesions (metastatic breast cacer with squamous differentiation) | PIK3CA | exon21 | c.3140A>G | p.H1047R | Class I variants | 72.9% |
TP53 | exon8 | c.818G>A | p.R273H | Class I variants | 60.9% | |
ERBB2 (HER2) | - | - | - | Class I variants | 5.8 | |
ETV6 | exon6 | c.1105C>T | p.R369W | Class II variants | 18.2% | |
NRG1 | exon1 | c.341A>T | p.D114V | Class III variants | 31.4% | |
SMARCA4 | exon31 | c.4441G>A | p.E1481K | Class III variants | 11.0% | |
ZFHX3 | exon9 | c.6332C>T | p.P2111L | Class III variants | 38.2% |
IHC | Immunohistochemical |
FISH | Fluorescence in Situ Hybridization |
NGS | Next-generation Sequencing |
CT | Computed Tomography |
PET/CT | Positron Emission Tomography/Computed Tomography |
VATS | Video-assisted Thoracoscopic Surgery |
MRI | Magnetic Resonance Imaging |
DCIS | Ductal Carcinoma in Situ |
HE | Hematoxylin and Eosin |
TKIs | Tyrosine Kinase Inhibitors |
ADC | Antibody-drug Conjugate |
DS-8201 | Trastuzumab Deruxtecan |
CNV | Copy Number Variation |
MBC | Metaplastic Breast Cancers |
TERT | Telomerase Catalytic Subun |
| [1] |
Swain S M, Shastry M, Hamilton E. Targeting her2-positive breast cancer: Advances and future directions [J]. Nat Rev Drug Discov, 2023, 22(2): 101-126.
HYPERLINK "
https://doi.org/" https://doi.org/10.1038/s41573-022-00579-0 |
| [2] |
Liang Y, Zhang H, Song X, et al. Metastatic heterogeneity of breast cancer: Molecular mechanism and potential therapeutic targets [J]. Semin Cancer Biol, 2020, 60: 14-27.
HYPERLINK "
https://doi.org/" https://doi.org/10.1016/j.semcancer.2019.08.012 |
| [3] | Shi Q, Xuhong J, Luo T, et al. Pik3ca mutations are associated with pathologic complete response rate to neoadjuvant pyrotinib and trastuzumab plus chemotherapy for her2-positive breast cancer [J]. Br J Cancer, 2023, 128(1): 121-129. |
| [4] | Wu Q, Li J, Zhu S, et al. Breast cancer subtypes predict the preferential site of distant metastases: A seer based study [J]. Oncotarget, 2017, 8(17): 27990-27996. |
| [5] | Hanker A B, Pfefferle A D, Balko J M, et al. Mutant pik3ca accelerates her2-driven transgenic mammary tumors and induces resistance to combinations of anti-her2 therapies [J]. Proc Natl Acad Sci U S A, 2013, 110(35): 14372-14377. |
| [6] | Berns K, Horlings H M, Hennessy B T, et al. A functional genetic approach identifies the pi3k pathway as a major determinant of trastuzumab resistance in breast cancer [J]. Cancer Cell, 2007, 12(4): 395-402. |
| [7] | Enane F O, Saunthararajah Y, Korc M. Differentiation therapy and the mechanisms that terminate cancer cell proliferation without harming normal cells [J]. Cell Death Dis, 2018, 9(9): 912. |
| [8] | Fisher E R, Palekar A S, Gregorio R M, et al. Mucoepidermoid and squamous cell carcinomas of breast with reference to squamous metaplasia and giant cell tumors [J]. Am J Surg Pathol, 1983, 7(1): 15-27. |
| [9] | Tan P H, Ellis I, Allison K, et al. The 2019 world health organization classification of tumours of the breast [J]. Histopathology, 2020, 77(2): 181-185. |
| [10] | Krings G, Chen Y Y. Genomic profiling of metaplastic breast carcinomas reveals genetic heterogeneity and relationship to ductal carcinoma [J]. Mod Pathol, 2018, 31(11): 1661-1674. |
| [11] | Rakha E, Toss M, Quinn C. Specific cell differentiation in breast cancer: A basis for histological classification [J]. J Clin Pathol, 2022, 75(2): 76-84. |
| [12] | Sihto H, Lundin J, Lundin M, et al. Breast cancer biological subtypes and protein expression predict for the preferential distant metastasis sites: A nationwide cohort study [J]. Breast Cancer Res, 2011, 13(5): R87. |
| [13] | Wang H, Xiang D, Liu B, et al. Inadequate DNA damage repair promotes mammary transdifferentiation, leading to brca1 breast cancer [J]. Cell, 2019, 178(1): 135-151. e119. |
| [14] | Juan L S, Freije A, Sanz-Gómez N, et al. DNA damage triggers squamous metaplasia in human lung and mammary cells via mitotic checkpoints [J]. Cell Death Discov, 2023, 9(1): 21. |
| [15] | Lloyd-Lewis B, Gobbo F, Perkins M, et al. In vivo imaging of mammary epithelial cell dynamics in response to lineage-biased wnt/β-catenin activation [J]. Cell Rep, 2022, 38(10): 110461. |
| [16] | Kaneko S, Takasawa K, Asada K, et al. Mechanism of erbb2 gene overexpression by the formation of super-enhancer with genomic structural abnormalities in lung adenocarcinoma without clinically actionable genetic alterations [J]. Mol Cancer, 2024, 23(1): 126. |
| [17] | Jiang Y, Jiang Y Y, Xie J J, et al. Co-activation of super-enhancer-driven ccat1 by tp63 and sox2 promotes squamous cancer progression [J]. Nat Commun, 2018, 9(1): 3619. |
APA Style
Qiu, Y., Lu, Y. (2025). Lung Metastasis of HER2-positive Breast Cancer with Squamous Cell Differentiation Phenotype: A Case Report. American Journal of Clinical and Experimental Medicine, 13(6), 170-176. https://doi.org/10.11648/j.ajcem.20251306.12
ACS Style
Qiu, Y.; Lu, Y. Lung Metastasis of HER2-positive Breast Cancer with Squamous Cell Differentiation Phenotype: A Case Report. Am. J. Clin. Exp. Med. 2025, 13(6), 170-176. doi: 10.11648/j.ajcem.20251306.12
AMA Style
Qiu Y, Lu Y. Lung Metastasis of HER2-positive Breast Cancer with Squamous Cell Differentiation Phenotype: A Case Report. Am J Clin Exp Med. 2025;13(6):170-176. doi: 10.11648/j.ajcem.20251306.12
@article{10.11648/j.ajcem.20251306.12,
author = {Yu Qiu and Yuanzhi Lu},
title = {Lung Metastasis of HER2-positive Breast Cancer with Squamous Cell Differentiation Phenotype: A Case Report},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {6},
pages = {170-176},
doi = {10.11648/j.ajcem.20251306.12},
url = {https://doi.org/10.11648/j.ajcem.20251306.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251306.12},
abstract = {Drug resistance, recurrence, and metastasis are the main challenges that can lead to treatment failure and deteriorate outcomes of patients with breast cancer. Breast cancer metastasizes to different organs and may present with different phenotypic features. However, the underlying mechanisms of phenotypic plasticity of breast cancer still remain unclear. We herein report a case of HER2-positive breast cancer in which the patient developed acquired therapeutic resistance following standard postoperative adjuvant chemotherapy combined with anti-HER2 targeted therapy. The patient initially responded to treatment; however, one year after completion of therapy, new bilateral pulmonary nodules emerged. Subsequent pathological examination confirmed metastatic carcinoma with a transdifferentiated squamous cell phenotype. Comprehensive biomarker analyses, including immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and next-generation sequencing (NGS), were performed on matched samples from the primary breast tumor and the corresponding lung metastatic lesions. Integrated diagnostic results confirmed that the pulmonary lesions were metastatic in origin from the breast, harboring HER2 amplification as well as PIK3CA and TP53 mutations. In contrast to the primary lesion, the metastatic lung lesions demonstrated acquisition of a squamous phenotype, accompanied by multiple chromosomal heterozygous/homozygous deletions and copy-number gain that may have contributed to this phenotypic transformation. Despite HER2 amplification, the pulmonary metastases showed negative HER2 protein expression, possibly reflecting tissue-specific gene expression differences. These findings provide new insights for the clinical management of HER2-positive breast cancer.},
year = {2025}
}
TY - JOUR T1 - Lung Metastasis of HER2-positive Breast Cancer with Squamous Cell Differentiation Phenotype: A Case Report AU - Yu Qiu AU - Yuanzhi Lu Y1 - 2025/12/17 PY - 2025 N1 - https://doi.org/10.11648/j.ajcem.20251306.12 DO - 10.11648/j.ajcem.20251306.12 T2 - American Journal of Clinical and Experimental Medicine JF - American Journal of Clinical and Experimental Medicine JO - American Journal of Clinical and Experimental Medicine SP - 170 EP - 176 PB - Science Publishing Group SN - 2330-8133 UR - https://doi.org/10.11648/j.ajcem.20251306.12 AB - Drug resistance, recurrence, and metastasis are the main challenges that can lead to treatment failure and deteriorate outcomes of patients with breast cancer. Breast cancer metastasizes to different organs and may present with different phenotypic features. However, the underlying mechanisms of phenotypic plasticity of breast cancer still remain unclear. We herein report a case of HER2-positive breast cancer in which the patient developed acquired therapeutic resistance following standard postoperative adjuvant chemotherapy combined with anti-HER2 targeted therapy. The patient initially responded to treatment; however, one year after completion of therapy, new bilateral pulmonary nodules emerged. Subsequent pathological examination confirmed metastatic carcinoma with a transdifferentiated squamous cell phenotype. Comprehensive biomarker analyses, including immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and next-generation sequencing (NGS), were performed on matched samples from the primary breast tumor and the corresponding lung metastatic lesions. Integrated diagnostic results confirmed that the pulmonary lesions were metastatic in origin from the breast, harboring HER2 amplification as well as PIK3CA and TP53 mutations. In contrast to the primary lesion, the metastatic lung lesions demonstrated acquisition of a squamous phenotype, accompanied by multiple chromosomal heterozygous/homozygous deletions and copy-number gain that may have contributed to this phenotypic transformation. Despite HER2 amplification, the pulmonary metastases showed negative HER2 protein expression, possibly reflecting tissue-specific gene expression differences. These findings provide new insights for the clinical management of HER2-positive breast cancer. VL - 13 IS - 6 ER -
Department of Pathology, The First Affiliated Hospital of Jinan University, Guangzhou, China
Department of Pathology, The First Affiliated Hospital of Jinan University, Guangzhou, China